
By Lambert Strether of Corrente.
With respect to “upticks” — Covid “upticks” going up, “plummets” going down — both Covid and the public health establishment (and the political class (and the press)) have form, well pictured in this maybe-famous chart:
I have been thinking about how different people interpret data differently. And made this xkcd style graphic to illustrate this. pic.twitter.com/a8LvlmZxT7
— Jens von Bergmann (@vb_jens) March 17, 2021
(I thought this was from XKCD, but it’s the original). So when I hear “uptick,” I think, from bitter experience and with the scientists on the right, “exponential growth.” Those on the right, I will call “exponentialists.” Most everyone else is on the left, with “going down,” “under control,” and “let’s do brunch.” Of course, you can’t reverse engineer the truth out of bullshit[1], so this time around, the let’s-just-go-ahead-and-call-them minimizers might be right. Nevertheless.
So I sat up when I saw stories coming across my feed that said there was an increase in Covid[2] wastewater detected in New York City (NYC). I always keep a watchful eye on NYC, not least because it has form: New York City was the epicenter of the first 2020 wave [3], which is reasonable, given its continued status as a global entrepôt. (Not only that, we know now that Omicron could have been brewed in New York, not South Africa.) But what about the instant case? Does wastewater data show that there is an increase (“rising,” “uptick,” “rebound”) in Covid in NYC? First, I will look at the press coverage. Then, I will look at the data, and a critique of that data, and briefly conclude.
The Press Coverage
Here is a list of the headlines:
June 1: High concentrations of COVID detected at all 14 New York City wastewater treatment plants CBS New York. This story doesn’t give any sourcing for the data at all. It does, however have this graphic:
So everybody retweets the story with the graphic, and this minimizer quote:
[P]ublic health officials say it’s too early to know if it’s the start of a full-blown COVID wave.
June 1: Is COVID back in NYC? Wastewater surveillance shows virus is rising Gothamist. Gothamist actually broke the story, and it’s the pick of the litter. Gothamist gives the source of the data: It’s from the NYS Wastewater Surveillance Network. (NYWSN). They also interviewed the dashboard maintainer:
When it comes to SAR-CoV-2, “we would expect New York City to potentially go first,” said Dr. David Larsen, a Syracuse University professor who runs the New York state wastewater surveillance network dashboard
(More from Larsen later.) They also interview Biobot (Nassau County only), and give some excellent minimizer quotes:
“We look at wastewater data really over time,” said NYC health commissioner Dr. Ashwin Vasan. “We need to look at it a little bit over longer time periods to draw any important inference.”
“It’s less about worry and more about preparation. COVID is here. It’s not going anywhere. We’re living with it,” Vasan said. “We have shown that we can start to regain a sense of normalcy and rebuild our city even with COVID still circulating.”
(I’m here for rebuilding NYC, and hence I’d expect to see Vasan pushing for ventilation. But, at least after a cursory search, no.) Gothamist is also points out that wastewater testing is our only reliable proxy for the spread of infection, since testing has been eliminated (or privatized. At an average of $45 a pop!)
June 1: Uptick in COVID-19 Found in NY Wastewater. Here’s What It Could Mean NBC New York. NBC gives the dashboard and cites to Gothamist. And Gothamist’s minimizing quote from Vasan!
June 1: NYC Wastewater Suggests COVID-19 Rebound: Could This Signify A New Wave? Medical Daily. Medical Daily cites to Gothamist, links NYWSN, and uses Vasan’s minimizing quote. They also undercut wastewater testing:
Meanwhile, Dr. Bruce Y. Lee, a professor at the CUNY School of Public Health, told Gothamist that wastewater data only gives a general idea of the virus spread in the community. It does not provide a much clearer picture than lab testing data.
Right, but the prospect of using lab testing data is now zero, which one would assume [hollow laughter] that a professor of public health would know.
June 2: High concentrations of COVID detected at all 14 New York City wastewater treatment plants CBS New York. Same as June 1, and just as bad.
June 2: COVID cases could be rising in NYC based on wastewater testing data Scripps. Does not cite to Gothamist, links to NYWSN, no quote from Vasan, quotes an exponentialist (!):
Infectious disease experts say trends are what stands out in wastewater detection for contaminants and other infectious properties. While the “absolute number might be debatable, that trend is always something that makes” experts pay attention, Dr. Peter Chin-Hong, an infectious diseases specialist, told ABC News.
June 2: US COVID activity stays low, but NYC sees rise in wastewater positives CIDRAP. Shockingly bad. Granted, this is a snippet in a news summary, but there should still be a link NYWSN:
New York City’s COVID activity appears to be on the rise, with all 14 of its wastewater treatment plants showing high concentrations of the virus, according to CBS News. However, data from the NYC Health shows that cases, hospitalizations, and deaths remain at very low levels.
As whoever at CIDRAP “edited” this must surely have know, case data is terrible, hospitalization lags, deaths lag even more, and wastewater is the best proxy for cases we have.
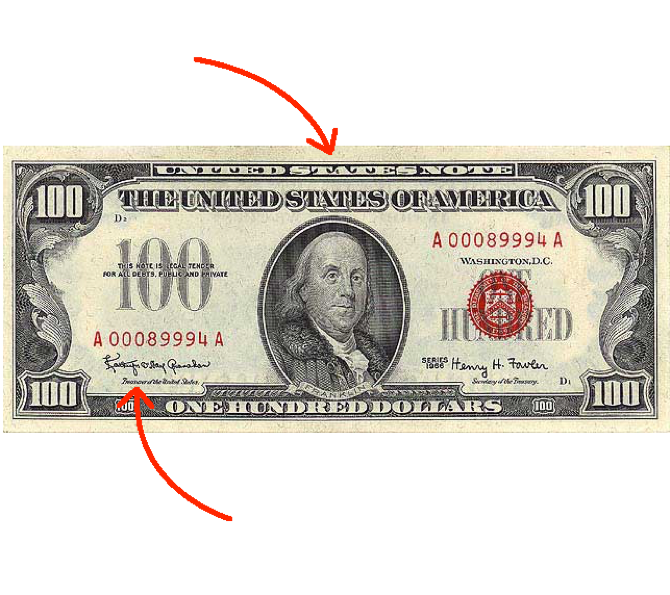
So that’s the media coverage. But is the coverage correct? One expert, at least, argues not:
So, when Topol amplified Weiland, was Topol correct? Let’s look at the data.
The Data
These are the sources I have[4]. In order, I will look at CDC, Biobot, the New York State Department of Health (NYSDH), and NYS Wastewater Surveillance Network (NYWSN). The stories all cite only to NYWSN, and that is the only data source that Topol (and Weiland) consider. In all cases, I have used data that indicates trends, not absolute numbers, since that’s the question: Is Covid rising in NYC?
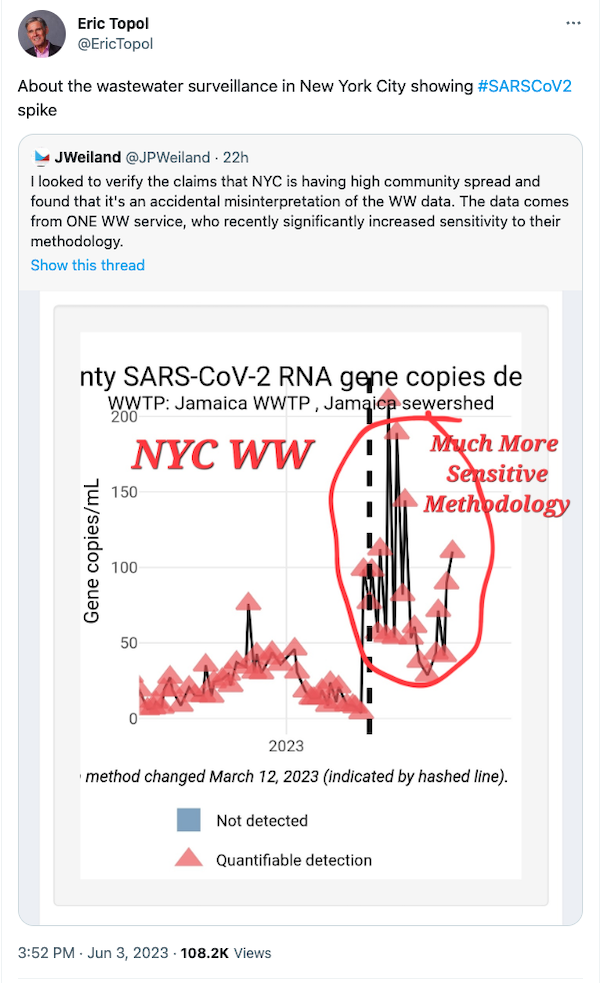
CDC. I am really including the CDC only to show how horrid their site is, and how hard they make it to get anything useful from it. Why on earth can’t I get an integrated view of all the counties at a reasonable size? Why can’t I drag the map around, and zoom in? Why does the server keep going down? So herewith:
Time Period: May 15, 2023 – May 29, 2023.
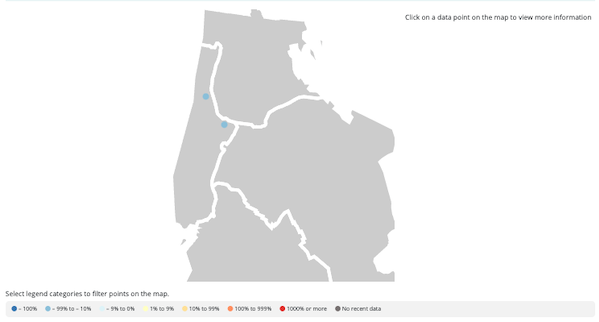


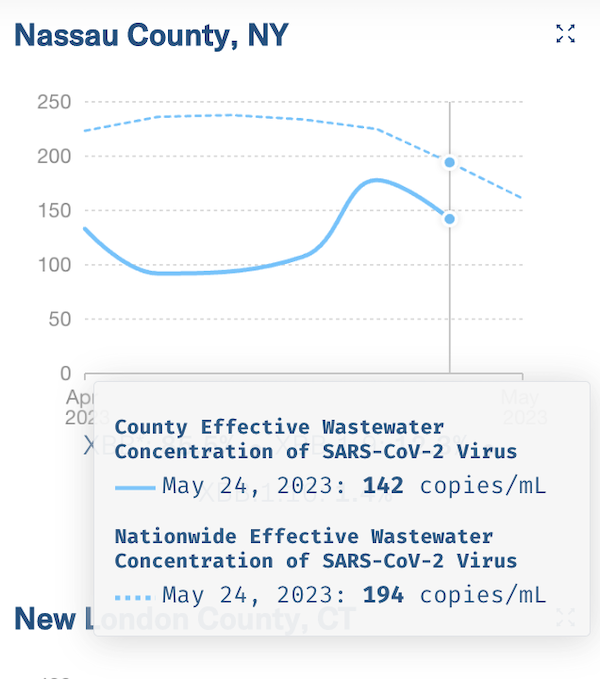
Biobot. I include the Biobot data mostly for grins. No knock on Biobot, but if NYC is throwing a signal, they’re not equipped to catch it. Their only site in New York is Nassau County:
Time Period: Data as of May 24.
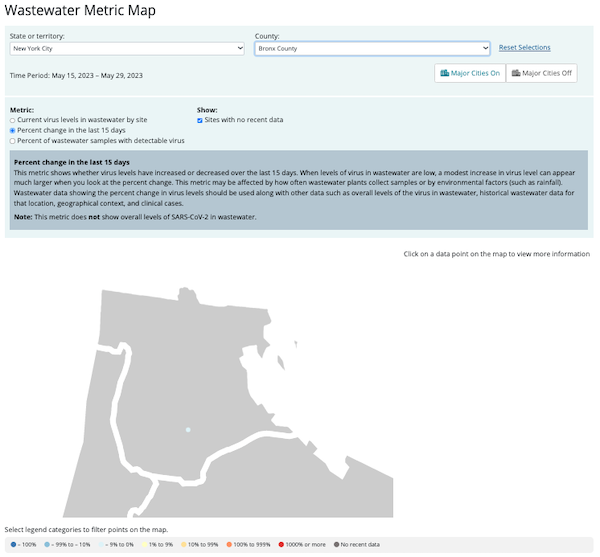
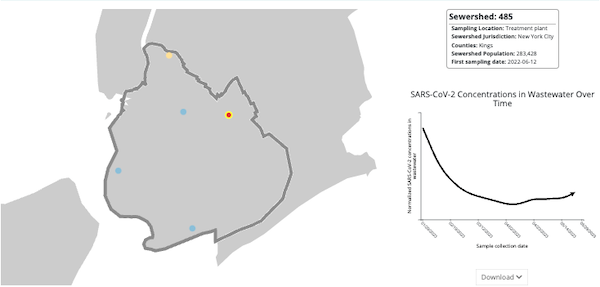
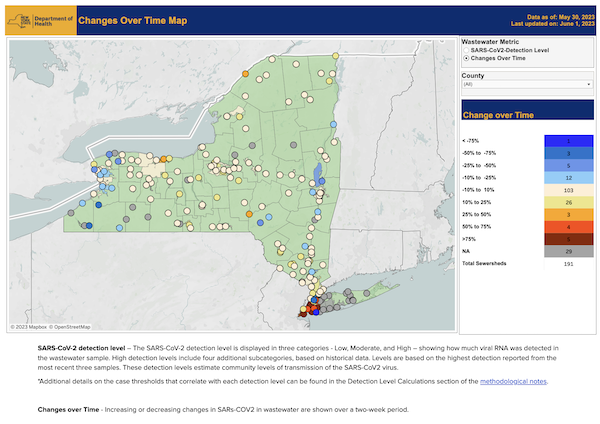
New York State Department of Health (NYSDH)
Time Period: Data as of May 30.
NYS Wastewater Surveillance Network (NYWSN)
Time period: Last Sample, June 1.
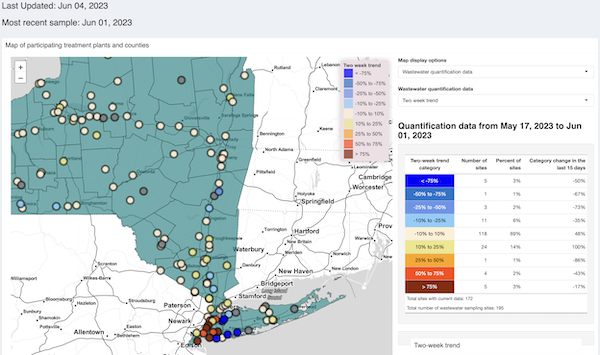
(Again, the source everyone cites.)
So, we can draw different conclusions from the data we have. CDC says there’s only one uptick, in King’s County (I can’t imagine why Topol didn’t check them before amplifying Weiland). Biobot can’t say whether there’s an uptick or not. NYSDH says there are upticks at multiple locations (see red dots). NYWSN agrees.
I am inclined to dismiss CDC’s data, first, because they’re CDC MR SUBLIMINAL Which should be jackhammered to rubble, the rubble plowed under, and the earth salted and I don’t trust them not to game the data, not after the “Green Map”, and second, because their sampling period ends the earliest. (If you have exponential spread, even one or two days will matter, depending on how infectious the variant is.) I am inclined to agree with NYSDH and NYWSN, not least because two separate teams using different algorithms came to the same conclusion. Weiland (amplified by Topol) critiques only NYSWN, so let’s look more closely at what he says:
First, NYSDH and NYWSN agree; Weiland (and Topol) have nothing to say about NYSDH data. Second, when Weiland says “recently increased sensitivity to their methodology,” “recently” is doing much more work than a poor adverb should have to do. The original Gothamist article — which everybody should have read, including Weiland and Topol — quotes the NYWSN maintainer:
In mid-March, the city switched to a more sensitive method for detecting coronavirus in wastewater, but that switch isn’t responsible for the new uptick, [Dr. David Larsen, a Syracuse University professor who runs the New York state wastewater surveillance network said.’
I don’t buy that a methodological change in March invalidates data [breaks out calculator] two months later, especially when other confirm it. Nor do I see why Topol, with Weiland, allows “recently” to get away with all that heavy lifting. Just to confirm that Gothamist quoted Larsen accurately, here is the NYWSN site:
Data for New York City’s five boroughs are analyzed by the City Health Department. Real-time reverse transcription quantitative polymerase chain reaction (RT-qPCR) was used for SARS-CoV-2 N1 gene copy determinations for samples collected August 31, 2020-March 7, 2023. Starting with samples collected on March 12,2023, digital reverse transcription quantitative polymerase chain reaction (dPCR) has been used. Due to differences in methodology, dPCR viral load values are ~10-20 times higher than RT-qPCR values. Therefore, increases in viral load between March 7th, 2023, and March 12, 2023 are due in part to changes in methods. The method change is noted on the raw gene copy plots for NYC sites with a hashed line on March 12, 2023.
The baseline changed in March. Today’s increase is relative to that new baseline. Weiland, called on this, goes straight to minimization:
Right, I don’t dispute that there might be an uptick (I wouldn’t call it a trend yet though, maybe after another week). However, levels are still ~10 TIMES lower than they were back in January. Overall levels remain very low in NYC relative to fall/winter.
— JWeiland (@JPWeiland) June 3, 2023
So what if the levels are “low” relative to January? This is the “Under Control” stage (at left) in the graphic I led with. Sheesh.
Conclusions
I conclude that there is in fact a Covid uptick in NYC. So, in a massive self-own, I’ve got to throw a flag on a Betteridge’s Law violation. As a confirmed exponentialist, if I were in NYC, I’d assume the worst. After all, how hard is it to mask up? And shpritz your Betadine or Enovid or whatever? Not hard at all.
I also conclude that the whole “personal risk assessment” schtick is demented. If this is what I have to do, to figure out if Covid is really increasing in NYC or not, nobody normal is doing to do it, and in fact nobody normal should have to (it’s just the sort of homework that PMCers like that sociopath Bob Wachter love. Who needs it?).
I would argue that your personal protocol should already be strong enough to deal with an uptick, or even a wave. The time to change your protocol is not when data changes, because the data is partial, certainly gamed (again, CDC’s infamous “green map”), might be lagging, might not be granular enough for your location, and might even be bad or non-existent. Change your protocol only when what you see in the material world changes: Where you see ventilation protections installed (it does happen, and I’m sure more often than we think). Or when a venue that was stone 3Cs changes for the better. Or when more people mask. Stay safe out there, and let’s save some lives!
NOTES
[1] Unless your heuristics are God-level, of course.
[2] Rather, an increase of the virus, SARS-CoV-2, but let’s not be pedantic.
[3] Interestingly, this post was impossible to find on Google, and very easy to find on Bing.
[4] I must update the listing in Water Cooler, which includes only NYWSN, and not the New York State Department of Health.
