

By Lambert Strether of Corrente.
This headline from CalMatters sums up where we are with so-called “public health” these days: “California ends COVID isolation rule for asymptomatic cases as winter infections climb.” They summarize the “rule” (really an “order”):
Californians infected with COVID-19 may go about their lives without isolating or testing negative as long as their symptoms are improving, according to new and significantly loosened guidelines from the California Department of Public Health [CDPH].
California’s top public health official, Dr. Tomás Aragón, last week quietly rescinded the state’s previous order, which encouraged people infected with COVID-19 to isolate for five days.
The new health order allows Californians with COVID-19 to return to work or school as long as their symptoms are improving and they are fever-free for 24 hours without medication. Asymptomatic individuals who test positive are not considered infectious and do not need to isolate, according to the order.
(This order is even laxer than CDC’s guidance.) No doubt NC readers are already shaking their heads, appalled, and I’ll go into some detail when I look at the wording of the Order proper.
Here are the problems I see with the CDPH order:
1) The Order guarantees infection with SARS-CoV-2, a Level Three Biohazard. This is a strange policy for a public health agency to adopt;
2) The Order, an “underground regulation,” violates California’s Administrative Procedures Act (APA);
3) The Order espouses a regulatory philosophy not justified in law.
Points (2) and (3) may justify a petition to California’s Office of Adminstrative Law (OAL). If the OAL decides in favor of the petitioner, then the Order would be unenforceable under the APA.
Here I must issue the following MR SUBLIMINAL Whinging caveat: IANAL (“I am not a lawyer”). What follows is my own best interpretation of the statutory and regulatory landscape, but I’m a layperson, California public health law is complex, and California adminstrative law is even more complex (which is why they have a whole office for it). For example: Is an order a regulation? Is a regulation a rule? Do Public Health Orders have a different legal regimen from other orders? Is a “State Public Health Officer Order” in the same bucket as a “Public Health Order”? Can these orders be derived from or over-ridden by a Governor’s executive order? I feel as if some sort of Shephardizing for administrative law is required here, and I don’t have the capacity.
Therefore, readers, please regard what follows as commonsensical, inspirational, and not definitive. Remember, though, what CalMatters said: The existing, more stringent order, was “quietly rescinded.” One can only wonder why! In what follows, we’ll unpack what “quiet” means.
The CDPH Order
Here is the the order: “State Public Health Officer Order for COVID-19 Disease Control & Prevention” (the “CDPH Order” or “Order”) issued January 9, 2027 by Dr. Tomás Aragón, and containing these stirring words:
NOW, THEREFORE, I, as State Public Health Officer of the State of California, order
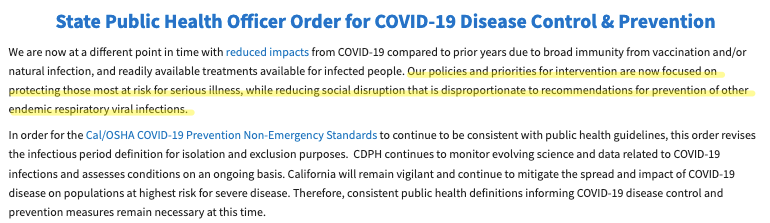
I’ll go into more detail in the next section, but for now check this out from the preamble (preceding “NOW….”):
Covid is not “endemic” like “other” “respiratory viral infections.” Neither the flu nor RSV produce the vascular and neurological damage that Covid does. Covid is far more lethal than either. We have Long Covid, but not Long Flu or Long RSV. In fact, there’s dispute as to whether SARS-CoV-2 should even be classified as a “respiratory virus”; its point of entry is the respiratory tract, but after that, it infects the entire body (creating, as we learned today, reservoirs of infection in bone marrow). I understand that public health has institutional imperatives (“efficiency”) that drive them to throw the Flu, RSV, and Covid into the “miscellaneous respiratory virus” bucket, but those imperatives are not health-related. Finally, according to Biobot wastewater data reinforced today, we’re in the second highest Covid transmission spike after Omicron. It’s absolutely disingenuous and tendentious to call Covid endemic. Now let’s turn to the Order.
The CDPH Order Guarantees Infection
Interestingly, the Order is sound on aerosol transmission, at least in theory; but in practice, it is not so sound. There are two sections to examine: “Close Contact” and “Infectious Period.” Both guarantee infection. Let us take each in turn.
First, “close contact.” From the Order:
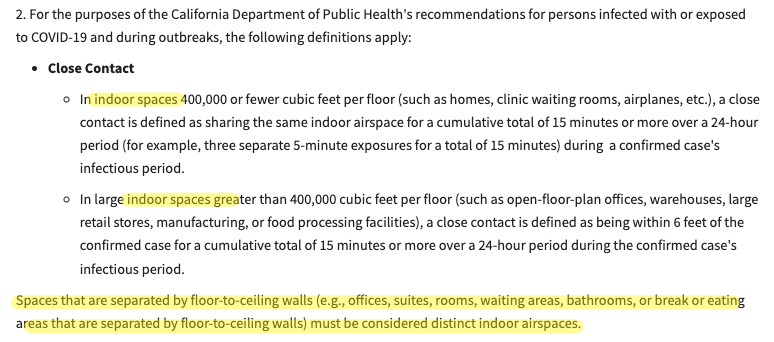
All this sounds great until you come to the definition of “distinct” “indoor spaces” at the end. In practice, what this means is that an asymptomatic doctor could be in close contact with a patient in their room, and then when they go out into the hall, they can unmask — if they masked at all — and the 15-minute clock resets! Or an infected doctor…. The same with patients; the clock resets when they leave their room, and go down the hall, say to the bathroom or for treatment in another room, when the clock resets again. In other words, the Order has no notion that SARS-CoV-2 can build up over time in the entire facility (which, since Covid spreads like smoke, is a given). That guarantees infection in the institutional population, including visitors and patients.
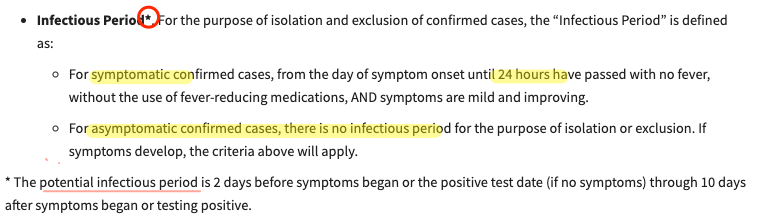
Second, “infectious period.” From the Order:
It’s well-known in the literature — and therefore to Aragón — that Covid transmits asymptomatically (Public Health: “Overall, asymptomatic transmission was 24.51%.” Studies differ, but in no case is asymptomatic transmission negligible). Aragón must also know that even the CDC admits that Covid’s infectious period lasts at least five days. Again, from the Biobot data, we’re in the second highest spike since Omicron.
The bottom line: By forcing infected children back to schools or infected workers back to work after one (1) day, and forcing the uninfected to share air with the infected, CPDH is guaranteeing infection[1]. (Perhaps the number of those infected could be reduced with a mask mandate, but CPDH says masking is only something to “consider.”) Herding people toward spaces where infection concentrates, like schools and the workplace, seems a strange goal for a public health agency. (CPDH seems to think they can eliminate asymptomatic infection with the stroke of a pen: “For asymptomatic confirmed cases, there is no infectious period… ” (!). And what’s with that asterisk? Apparently, the “potential infectious period” is two days before symptoms through ten days after, but that’s not the real infectious period? What does that even mean? “I’m infected, but with an asterisk“?) And with that, let’s turn to the legalities.
The CDPH Order Is An “Underground Regulation”, Hence Unenforceable
What is the status of the CDPH Order? It looks to me very much like an “Underground Regulation” — remember “quietly rescinded?” Most things done underground are quiet — defined by the OAL as follows:
State agencies, with few exceptions, are required to adopt regulations following the procedures established in the Administrative Procedure Act (APA). A regulation is defined in Government Code section 11342.600:
“Regulation means every rule, regulation, order, or standard of general application[A] or the amendment, supplement, or revision[B] of any rule, regulation, order, or standard adopted by any state agency[C] to implement, interpret, or make specific the law enforced or administered by it[D], or to govern its procedure[E].”
So, “orders” fall into the “Regulation Bucket.”[2] Importantly:
If a state agency issues, utilizes, enforces, or attempts to enforce a rule without following the APA when it is required to, the rule is called an “underground regulation.” State agencies are prohibited from enforcing underground regulations.
The CPDH, as best I can determine, has violated at least three APA requirements in publishing the Order, making the Order an “Underground Regulation.” As you can see by reading the Order on the CPDH site, the Order (1) is missing a unique identification number; (2) the CDPH web site is out of compliance; further, (3) there was no hearing under the Bagley-Keene Act before the Order was promulgated. (Yves used Bagley-Keene to great effect while skewering those corrupt dolts at CalPERS). Taking these in order:
(1) Here is the relevant text from the APA on a unique identification number:

The Order has no such ID. An activist called the OAL, and was told that that “CDPH didn’t register [the Order] with a regulation number.”
(2) Here is the relevant text from the APA on the web site;
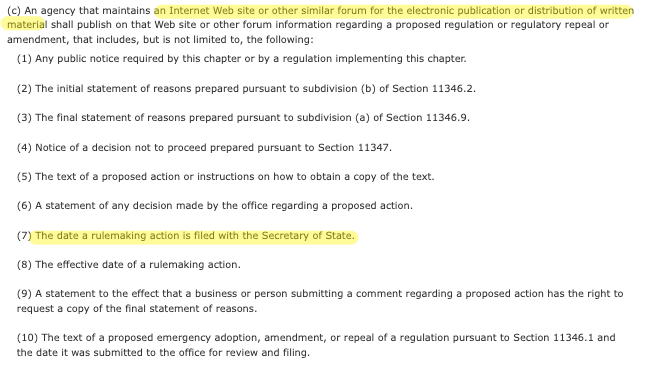
The web page does not contain the date the “rule-making action” (“regulation”) was filed with the Secretary of State (#7), although it does contain an effective date (#8).
(3) Finally, no there was no public meeting held before the Order was putatively put into effect. If a public meeting was required, it would have been required by the Bagley-Keene Act. Before digging in, let me quote the glorious opening section, 11120:
It is the public policy of this state that public agencies exist to aid in the conduct of the people’s business and the proceedings of public agencies be conducted openly so that the public may remain informed.
In enacting this article the Legislature finds and declares that it is the intent of the law that actions of state agencies be taken openly and that their deliberation be conducted openly.
The people of this state do not yield their sovereignty to the agencies which serve them. The people, in delegating authority, do not give their public servants the right to decide what is good for the people to know and what is not good for them to know. The people insist on remaining informed so that they may retain control over the instruments they have created.
Hopefully, the people have retained control over decision-making by a public health body during a pandemic. Moving into the detail — that is, for a non-lawyer, beginning to juggle the snarling chain-saws — the key section seems to be 11122.5:
11122.5. (a) As used in this article, “meeting” includes any congregation of a majority of the members of a state body at the same time and place to hear, discuss, or deliberate upon any item that is within the subject matter jurisdiction of the state body to which it pertains.
(b) (1) A majority of the members of a state body shall not, outside of a meeting authorized by this chapter, use a series of communications of any kind, directly or through intermediaries, to discuss, deliberate, or take action on any item of business that is within the subject matter of the state body.
In other words, as CDPH deliberated on revising the Order, they would have had to do so in a public meeting, and not privately. The only reason that would not be so is if CDPH were not a “state body,” which seems absurd. However, there is, in fact, a potential exemption to that effect at 11121.1:
As used in this article, “state body” does not include any of the following:…
(e) State agencies provided for in Section 109260 of the Health and Safety Code [HSC], except as provided in Section 109390 of the Health and Safety Code.
I believe that in fact the CDPH is governed by the HSC, or its ability to regulate is; but when I looked at the exemptions in sections 109260 and 109390 they didn’t seem relevant.
So, at least as far as I can tell, the Order was governed by Bagley-Keene. There should have been a meeting, and it should have been public. But there was no meeting. (I am told by a reliable authority that claims of Bagley-Keene violations must be filed within 90 days of the violation.)

(Yes, this is only one month, but I looked back to September.) So that’s what “quiet” means. No public meetings!
Hence, there are three reasons why the Order is an “Underground Regulation,” and OAL should stop it from being enforced, which they can do, if some kind soul files a petition to that effect.
CDPH Regulatory Philosophy is not Justified in Law
The order ends with the following intriguing sentence:
![]()
I went through all these sections of the HSC. Here they are. I have helpfully underlined the problematic sections:
120125: “The department shall examine into the causes of communicable disease in man and domestic animals occurring or likely to occur in this state.”
120140: “Upon being informed by a health officer of any contagious, infectious, or communicable disease the department may take measures as are necessary to ascertain the nature of the disease and prevent its spread. To that end, the department may, if it considers it proper, take possession or control of the body of any living person, or the corpse of any deceased person.”
120175: “Each health officer knowing or having reason to believe that any case of the diseases made reportable by regulation of the department, or any other contagious, infectious or communicable disease exists, or has recently existed, within the territory under his or her jurisdiction, shall take measures as may be necessary to prevent the spread of the disease or occurrence of additional cases.”
120195: “Each health officer shall enforce all orders, rules, and regulations concerning quarantine or isolation prescribed or directed by the department.”
131080: “The department may advise all local health authorities, and, when in its judgment the public health is menaced, it shall control and regulate their action.”
But here is what the Order is designed to do:
The statutes justifying the Order say “prevent the spread.” That is their plain meaning. The statutes do not say “prevent the spread while reducing social disruption.”[3] The nature and level of “social disruption” is, I would argue, a political question — hence the title of this post — and the statutes do not justify political engagement by the CDPH.
Conclusion
I apologize for the extremely dry nature of this post, whose juicy subject is, after all, how many members of the unwitting public the public health establishment will be able to force under the bus. I hope some of the ideas expressed here will inspire activists with more legal acumen than I possess to continue their good work, and file a petition against the Order with the OAL. I hope they have success similar to those activists who forced CDC to rethink HICPAC’s attempt to make patient protections in hospitals worse then they were before the pandemic began.[4]
NOTES
[1] DCPH even knows this. KQED:
[CDPH] in an email to KQED, elaborated that “a significant proportion of COVID-19 infections are asymptomatic or include minimal symptoms, and many people may be infected with COVID-19 or other respiratory infections and do not test or know what infection they may have.”
[2] An anonymous source — anonymous because of my caveats; I don’t want to embarass them! — threw the following over the transom, keying the wording of the Order (marked by square brackets, thus: [A], and italicized) to a showing that Government Code section 11342.600 applies:
[A] Rule, Regulation, Order, or Standard of General Application:
The COVID-19 Isolation Guidance issued by the CDPH on January 9, 2024, is a rule, regulation, order, or standard that applies to the general population of California. It provides specific guidelines and requirements for individuals who need to isolate due to COVID-19 infection or exposure.
[B] Amendment, Supplement, or Revision
By issuing the update on January 9, 2024, the CDPH is amending, supplementing, or revising the existing COVID-19 Isolation Guidance that was previously in effect. The update is intended to provide further clarification, modifications, or additions to the previous guidance, thereby altering the previous requirements and obligations imposed upon individuals subject to isolation measures.
[C] Adopted by a State Agency:
The COVID-19 Isolation Guidance update was issued by the California Department of Public Health, which is a state agency responsible for enforcing and administering public health laws within the state. As such, the update is adopted by a state agency and falls within the jurisdiction and authority of the CDPH.
The California Department of Public Health guideline was further incorporated into a regulation of Cal/OSHA, a division of the State of California Department of Public Relations, which is a state agency, on the same date of January 9, 2023, and is explicitly stated on the regulation that “These regulations apply to most workers in California who are not covered by the Aerosol Transmissible Diseases standard.”
[D] Implements, Interprets, or Makes Specific the Law Enforced or Administered by the CDPH and Cal/OSHA:
The COVID-19 Isolation Guidance update is issued by the CDPH to implement and provide specific guidelines for the enforcement and administration of public health laws related to COVID-19. It clarifies the requirements for individuals who must isolate due to infection or exposure, thereby making specific the obligations imposed by the public health laws enforced by the CDPH.
[E] Governs Procedure:
The January 9, 2024, update on COVID-19 Isolation Guidance includes procedural instructions and protocols that individuals must follow when isolating. It outlines the steps to be taken, such as testing, duration of isolation, monitoring symptoms, and when it is safe to discontinue isolation. Therefore, the guidance governs the procedure that individuals must adhere to when undergoing isolation, making it a regulation within the defined scope.
An exception might be claimed if the CDPH was issued during the period of time during California’s COVID-19 State of Emergency. Due to special conditions under that Emergency Order. However, the emergency order has ended as of Feb 28, 2023 and does not provide a basis for exemption.
[3] The ideological position that public health is a matter of striking a balance between mordidity and mortality in the population and social disruption is pervasive in the public health establishment, no doubt because of the political and institutional power it brings. This version of Rule #2 was expressed in particularly vicious and reprehensible form, as we would expect, by Tufts University Infection Control [sic] officer Shira Doron (co-author of this infamous paper with HICPAC member Erica Shenoy):
“The question is, is the juice worth the squeeze?” said Dr. Shira Doron, chief infection control officer for the Tufts Medicine health system in Massachusetts. “We’re not achieving containment of the virus. So what are we getting from this policy?”
Of course, it’s not Doron’s “juice” that’s being “squeezed.” And we’re not “achieving containment” due to a catastrophic failure by the public health establishment, which they, including Doron, continue with increasing desperation to reinforce. But here we are!
[4] Where the heck are the unions on this?
